
Asthma is treated firstly, to remove or lessen its symptoms and agony, and secondly, to remove its cause as far as possible. It is better and desirable that both aspects be undertaken side by side. Let us first take the drug treatment of asthma.
As we have already seen, a patient of asthma during an attack has constriction of the airways and excessive production of lung secretions. The narrowed airways make respiration and exchange of gases in the lungs difficult, so that the patient has less of the oxygen and more of carbon dioxide in his blood.
The excessive secretions can within a shortwhile lead to infection in the lungs, as the secretions are the nutrients of the different kind of bacteria and they grow very fast on it.
Furthermore, since a patient having an attack of asthma breathes very fast, he loses lot of water in the air which he throws out, and so loses, a lot of water from his body.
Treatment During an Attack
- If the attack is very severe and prolonged, leading to deficiency of oxygen in the blood, which can be clinically ascertained by looking for bluish tinge on the body, tongue or conjunctivae, then administration of oxygen through nose is called for.
- The constriction of the airways has to be removed and production of excessive secretion stopped.
- If there are signs of infection in the lungs, appropriate antibiotics are to be given.
- If the patient is dehydrated, intravenous 5 per cent glucose-saline is to be given.
Let us take up these items in more detail. Giving of Theophylline tablets, 2 tablets twice or thrice a day, depending upon the age, weight and severity of the condition, proves very helpful. Theophylline retard or sustained action tablets are also available.
The simplest and the well-tried drug combination for causing dilatation of the airways is giving a tablet which contains ephedrine, aminophylline and phenobarbitone. This combination is available under different proprietory names such as Tedral, Franal etc. This can be repeated two or three times a day. For children, syrups are available containing this combination.
For most patients having mild or moderate attack of asthma, this proves very helpful and even adequate in itself. Some patients do complain of palpitation after taking these tablets, and older patients having high blood pressure have to take it in lesser quantities. Ephedrine in it can cause constipation and if the patient has some enlargment of the prostate, it can cause some difficulty in passing urine. But generally speaking, such tablets prove very efficacious.
Drugs like salbutamol (which are B-2 stimulators) have come into use lately. They specifically dilate the bronchial airways without excessively stimulating the heart, so that they do not usually lead to palpitation. These drugs come in the form of tablets, injections or aerosol inhalers. In combination with deriphylline, salbutamol tablets prove very useful.
In case there is a severe attack of asthma, deriphylline injection given intramuscularly or aminophylline with 5 per cent glucose intravenously, slowly in 5 to 10 minutes proves helpful. Aminophylline given through intravenous drip with 5 per cent glucose is very useful. An injection of adrenaline (1:1000 solution) ½ ml, given very slowly subcutaneously, is also effective in many cases.
Most patients usually need only this medication and care. But, at times, the symptoms increase or when an infection supervenes, extra care is needed. If bacterial infection is present in the respiratory passages and unless properly and adequately treated, bronchodilator drugs either exert diminished action or have no action at all, so that the patient keeps getting breathless. So, as far as possible, the causative organism must be identified, its sensitiveness to a drug found, and then the proper drug administered.
But in the majority of the cases, this is not possible either because of the lack of facilities or the procedure takes more time than a patient can afford. In such a situation, ampicillin has been found to be helpful: one or two capsules of 250 mg thrice a day for a week proves adequate; the dose and length of administration depends, however, upon the severity of infection.
If the attack of asthma is such that it is not controlled by the bronchodilator tablets, injections as well as the antibiotics, then the patient can be put on corticosteroids. These can be given as tablets or intramuscularly or in very severe cases, intravenously.
Treatment in Status Asthmaticus
If the patient has been in status asthmaticus (i.e., continuous and severe attack of asthma for more than 24 hours), it is important to keep in mind that he may also be dehydrated because of excessive loss of water from the lungs; by excessive perspiration and by omitting to take fluids while in an attack. Hence his fluid loss has to be replaced adequately. This besides restoring the fluid balance of the body, lessens the thickness of the tenacious sputum so that it is coughed out easily. In such a case, intravenous fluids are administered early, usually 3 to 5 litres in the first 24 hour period, and thereafter 3 litres daily until hydration is achieved. Fluids usually consist of 5 per cent dextrose in water; every second or third such fluid should contain sodium chloride, particularly if prolonged intravenous therapy in necessary, or if the patient is perspiring freely and he vomits or has diarrhoea. As the patient becomes hydrated and starts eating well, the intravenous administration of fluids can be curtailed.
A cyanosed patient of asthma in status asthmaticus is in need of oxygen which must be given. This can be given either through a catheter in the nose or through a ventri-mask or through a positive pressure breathing apparatus along with a bronchodilator; the last mode of therapy has proved to be more effective.
The use of expectorants in the management of asthma is one of the most important yet often neglected aspects of treatment. One of the best expectorants is potassium iodide; when it is tolerated poorly, other substances such as glyceral guiacolate and ammonium chloride may be useful. Water vapour also may be helpful in thinning bronchial secretions.
Patients with severe asthma become profoundly exhausted, lose sleep, experience increasing anxiety, and therefore, are in need of a tranquilliser, but is should be kept to a minimum, because excess of it can interface with respiration.
Deaths from asthma can occur in spite of the antibiotics and steroids. These occur not only in older people who die of the complications of long-standing asthma, but also in younger people aged between 5 and 35 years. Majority of these deaths occur outside the hospital. These are due to the fact that the patient and his relatives could not realise the severity of the situation.
A proper understanding of the patient’s fears and anxieties and the allaying of these fears through sympathetic coversation helps asthma patients very much. The majority of these patients are prone to suggestion. It has been seen, time and again, that when a prescription is given or a line of treatment is started with the emphatic suggestion to the patient that this will definitely give relief, it decidedly works and the patient fulfils the expectations. Not only that, I have observed, that with whatever symptoms the patient looks better, produces a corresponding response and the hope given that “You will imporve still further”, works miracle. Such an approach is helpful, but care must be taken because over-optimistic hopes, once shattered, cause more harm than good.
Aerosol Inhalers
Aerosol are the solid or liquid particles of a substance suspended in air. They are very small, less than a micron (1/1000 mm) in size.
Aerosol inhalers were used initially with bronchodilator drugs like Isoprenaline. But because this drug caused many side-effects such as palpitation and dizziness and some deaths too due to frequent use, this mode of treatment fell into some disrepute.
With the availability of aerosol inhalers with salbutamol and corticosteroids, this form of treatment has become now very popular.
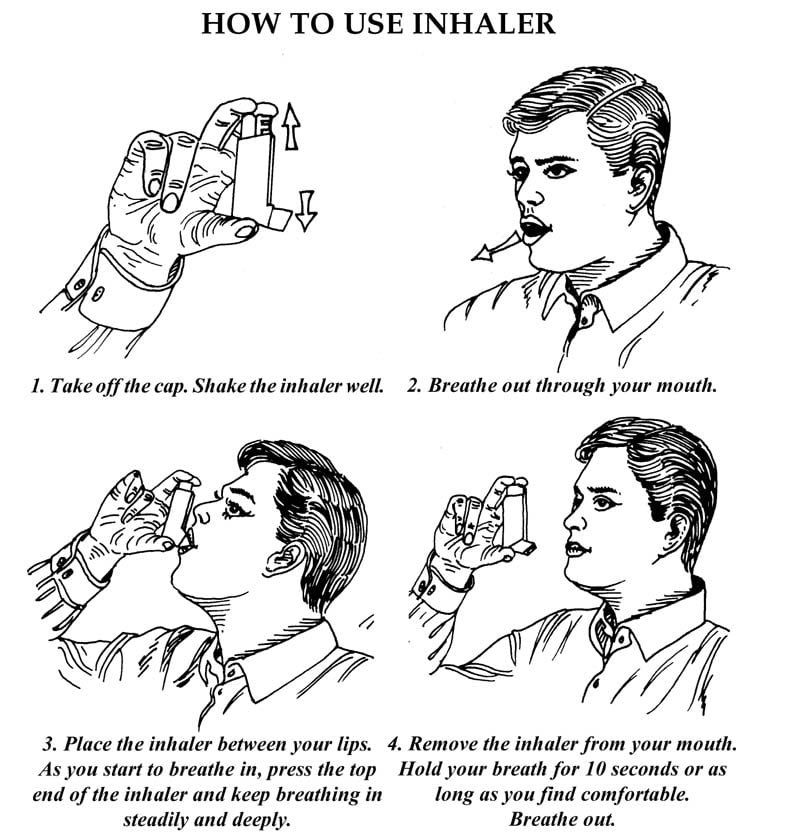
The technique of using the inhaler is as follows:
- Shake the inhaler. Remove the cap from its mouth-piece. Insert the mouth-piece in the lips and purse the lips tightly around it
- Take one or two breaths with the inhaler in the mouth.
- Exhale completely, and then as you start inhaling, press the nozzle-button of the inhaler. Aerosol would go in the airways alongwith the air inhaled.
- Now remove the inhaler from the mouth. Keep the lips closed, and hold the breath as long as possible, then open the mouth.
- You can repeat the process and take one more does of aerosol from the inhaler. The dose that comes out each time on pressing the inhaler equal and is measured.
Cortisone
Cortisone, the miracle drug, has provided renewed hopes to the patient suffering from very severe forms of allergies including asthma. This is a very potent drug and ought to be used in acute life-threatening situations. In asthma cases, cortisone can help patients where nothing else helps, but then it ought to be used only when everything else has been tried and has failed.
It is difficult to say which manifestation of allergy are helped the most, but it is the asthma patients who make maximum use of them.
Among the asthma patients, corticosteroids have provided the maximum and most-needed relief to those having status asthmaticus. Intramuscular or intravenous administration abolishes symptoms in those patients in whom adrenaline or aminophylline have not been of much use. After corticosteroid administration, some of the patients who previously did no respond to adrenaline or aminophylline start responding can be resorted to. Gradually the corticosteroids can be tapered off and the patient can be put on other routine bronchodilators.
Short term use of corticosteroids has proved very helpful to those asthma patients who do not do well with the usual bronchodilators or to those who do not get adequate relief from them.
With the dosage and time for which these drugs are usually prescribed, no serious side effects or complications are observed. Complaints of general weakness or epigastric distress or diminished appetite are encountered when patients are given ephedrine and aminophylline.
Acute attacks not responding to other routine measures, show excellent improvement in seasonal asthma cases. On the other hand, perennial asthmatic cases who have developed irreversible structural changes in the lungs, do not respond very well.
Care in Administration : The conditons generally forbid the use of cortisone are diabetes mellitus, pepticulcer, gastrointestinal bleeding, tuberculosis, psychosis, old age, chronic kidney disease, heart attack and significant hypertension. However, these contra-indications are more relative than absolute. Long-term taking of corticosteroids may produce hairiness (hirsutism) over the face.
While corticosteroids are being taken, an acute infection in the body does not produce as much symptoms as it would do otherwise. Hence, if the symptoms of an infection are even minor, a doctor ought to be consulted.
Upon discontinuation of the corticosteroids, or on a too rapid decrease dosage, some patients complain of tiring easily, weakness, nervousness, irritability, gastro-intestinal disturbances and occasional dizziness.
Cortisone Inhaler : In cases of intractable asthma where other medications have failed or have not provided adequate relief and cortisone tablets have to be taken, cortisone inhaler reduces the need for the tablets. Since the inhaled cortisone acts locally in the lungs, it hardly produces any side-effects. The inhaler is needed to be used 3 to 4 times a day and provides appreciable relief.
Inhalations of cortisone on heavy dosage and for long periods can be lead to growth of fungi in the throat, causing soreness and discomfort. If it happens, the inhalations have to be stopped.
Antihistamines in Asthma
Antihistamines are not effective in the case of asthma in adults. They have no effect on bronchospasm; in fact, the symptoms sometimes get aggravated because of the drying up of the secretions and the subsequent difficulty in passing phlegm. Allergic cough in children, however, is helped by giving antihistamines along with a bronchodilator in cough mixture.
Any drug taken should be in consultation with your doctor.
Inhalation devices you can use
A few popular inhaltion devices are descibed here under:
Powder Inhaler
Powder Inhalers are devices that deliver a measured dose of medicine in a powdered form. The transparent Rotahaler is one such device. It uses a capsule to deliver the medicine and is very easy to use.
Spray Inhaler
The Spray Inhaler is the most widely used inhalation device in the world. It delivers a measured dose of medicine through a pressurised spray. To get the full benefit from a spray inhaler, it is essential to use it in a proper way.
Spacer
The spacer is a holding chamber which can be attached to the Spray Inhaler. It makes the Spray Inhaler easier to use and adds to its effectiveness.
Nebuliser
Nebulisers are used for giving higher doses of medication at times when breathing becomes very difficult. They are machines that transform the medicine into a fine mist, which can be breathed in by normal breathing, via a facemask or a mouthpiece. Nebulisers are usually used in hospitals and nursing homes, for the management of severe attacks.